


A Brief History of Mental Illness and the U.S. Mental Health Care System
The history of mental illness in the United States is a good representation of the ways in which trends in psychiatry and cultural understanding of mental illness influence national policy and attitudes towards mental health. The U.S. is considered to have a relatively progressive mental health care system, and the history of its evolution and the current state of the system will be discussed here.
Early History of Mental Illness
Many cultures have viewed mental illness as a form of religious punishment or demonic possession. In ancient Egyptian, Indian, Greek, and Roman writings, mental illness was categorized as a religious or personal problem. In the 5th century B.C., Hippocrates was a pioneer in treating mentally ill people with techniques not rooted in religion or superstition; instead, he focused on changing a mentally ill patient’s environment or occupation, or administering certain substances as medications. During the Middle Ages, the mentally ill were believed to be possessed or in need of religion. Negative attitudes towards mental illness persisted into the 18th century in the United States, leading to stigmatization of mental illness, and unhygienic (and often degrading) confinement of mentally ill individuals.
Mental Health Hospitals and Deinstitutionalization
In the 1840s, activist Dorothea Dix lobbied for better living conditions for the mentally ill after witnessing the dangerous and unhealthy conditions in which many patients lived . Over a 40-year period, Dix successfully persuaded the U.S. government to fund the building of 32 state psychiatric hospitals.
How was mental health treated in the 1900s?
The use of social isolation through psychiatric hospitals and “insane asylums,” as they were known in the early 1900s, were used as punishment for people with mental illnesses.
Mental Health America (MHA), originally founded by Clifford Beers in 1909 as the National Committee for Mental Hygiene, works to improve the lives of the mentally ill in the United States through research and lobbying efforts. A number of governmental initiatives have also helped improve the U.S. mental healthcare system .
When was mental health taken seriously in the US?
In 1946, Harry Truman passed the National Mental Health Act, which created the National Institute of Mental Health and allocated government funds towards research into the causes of and treatments for mental illness.
This institutional inpatient care model, in which many patients lived in hospitals and were treated by professional staff, was considered the most effective way to care for the mentally ill. Institutionalization was also welcomed by families and communities struggling to care for mentally ill relatives. Although institutionalized care increased patient access to mental health services, the state hospitals were often underfunded and understaffed, and the institutional care system drew harsh criticism following a number of high-profile reports of poor living conditions and human rights violations. By the mid-1950s, a push for deinstitutionalization and outpatient treatment began in many countries, facilitated by the development of a variety of antipsychotic drugs. Deinstitutionalization efforts have reflected a largely international movement to reform the “asylum-based” mental health care system and move toward community-oriented care, based on the belief that psychiatric patients would have a higher quality of life if treated in their communities rather than in “large, undifferentiated, and isolated mental hospitals”.
Although large inpatient psychiatric hospitals are a fixture in certain countries, particularly in Central and Eastern Europe, the deinstitutionalization movement has been widespread, dramatically changing the nature of modern psychiatric care. The closure of state psychiatric hospitals in the United States was codified by the Community Mental Health Centers Act of 1963, and strict standards were passed so that only individuals “who posed an imminent danger to themselves or someone else” could be committed to state psychiatric hospitals. By the mid-1960s in the U.S., many severely mentally ill people had been moved from psychiatric institutions to local mental health homes or similar facilities. The number of institutionalized mentally ill patients fell from its peak of 560,000 in the 1950s to 130,000 by 1980. By 2000, the number of state psychiatric hospital beds per 100,000 people was 22, down from 339 in 1955. In place of institutionalized care, community-based mental health care was developed to include a range of treatment facilities, from community mental health centers and smaller supervised residential homes to community-based psychiatric teams.
Why did mental health hospitals disappear in the US?
In the 1960s, laws were changed to limit the ability of state and local officials to admit people into mental health hospitals. This lead to budget cuts in both state and federal funding for mental health programs. As a result, states across the country began closing and downsizing their psychiatric hospitals.
In 1963, Congress passed the Mental Retardation Facilities and Community Health Centers Construction Act, which provided federal funding for the development of community-based mental health services.
Though the goal of deinstitutionalization – improving treatment and quality of life for the mentally ill – is not controversial, the reality of deinstitutionalization has made it a highly polarizing issue. While many studies have reported positive outcomes from community-based mental health care programs, (including improvements in adaptive behaviors, friendships, and patient satisfaction,) other studies have found that individuals living in family homes or in independent community living settings have significant deficits in important aspects of health care, including vaccinations, cancer screenings, and routine medical checks. Other studies report that “loneliness, poverty, bad living conditions, and poor physical health” are prevalent among mentally ill patients living in their communities. However, some studies argue that community-based programs that have proper management and sufficient funding may deliver better patient outcomes than institutionalized care, and are “not inherently more costly than institutions”.
Critics of the deinstitutionalization movement point out that many patients have been moved from inpatient psychiatric hospitals to nursing or residential homes, which are not always staffed or equipped to meet the needs of the mentally ill. In many cases, deinstitutionalization has also shifted the burden of care to the families of mentally ill individuals, though they often lack the financial resources and medical knowledge to provide proper care. Others argue that deinstitutionalization has simply become “trans-institutionalization”, a phenomenon in which state psychiatric hospitals and criminal justice systems are “functionally interdependent”. According to this theory, deinstitutionalization, combined with inadequate and under-funded community-based mental health care programs, has forced the criminal justice system to provide the highly structured and supervised environment required by a minority of the severely mentally ill population.
Opponents of the trans-institutionalization theory contend that it applies to a small fraction of mentally ill patients, and that the majority of patients would benefit from improved access to quality community-based treatment programs, rather than from an increase in the number of inpatient state psychiatric beds. These opponents claim that the reduced availability of state hospital beds is not the cause of the high rates of incarceration among the mentally ill, arguing that deinstitutionalized patients and incarcerated individuals with serious mental illnesses are “clinically and demographically distinct populations”. Instead, they suggest that other factors such as “the high arrest rate for drug offenses, lack of affordable housing, and underfunded community treatment” are responsible for the high rates of incarceration among the mentally ill.
Though the deinstitutionalization debate continues, many health professionals, families, and advocates for the mentally ill have called for a combination of more high-quality community treatment programs (like intensive case management) and increased availability of intermediate and long-term psychiatric inpatient care for patients in need of a more structured care environment. Many experts hope that by improving community-based programs and expanding inpatient care to fulfill the needs of severely mentally ill patients, the United States will achieve improved treatment outcomes, increased access to mental health care, and better quality of life for the mentally ill.
How was mental illness treated in the 1970s?
In the treatment of mental disorders, the 1970s was a decade of increasing refinement and specificity of existing treatments. There was increasing focus on the negative effects of various treatments, such as deinstitutionalization, and a stronger scientific basis for some treatments emerged.
The National Alliance for the Mentally Ill was founded in 1979 to provide “support, education, advocacy, and research services for people with serious psychiatric illnesses”. Other government interventions and programs, including social welfare programs, have worked to improve mental health care access.
Which president ended mental institutions?
President Ronald Reagan
In 1981 President Ronald Reagan, who had made major efforts during his Governorship to reduce funding and enlistment for California mental institutions, pushed a political effort through the U.S. Congress to repeal most of MHSA. The MHSA was considered landmark legislation in mental health care policy.
…
Mental Health Systems Act of 1980.
| Enacted by | the 96th United States Congress |
| Citations | |
|---|---|
| Public law | Pub.L. 96-398 |
| Codification |
The Omnibus Budget Reconciliation Act of 1981, signed by President Ronald Reagan on August 13, 1981, repealed most of the MHSA. The Patients’ Bill of Rights, section 501, was not repealed; per Congressional record, the Congress felt that state provisions were sufficient and section 501 served as a recommendation to states to review and refine existing policies.
Barriers to Mental Health Care
Due to the complex nature of psychological disorders, successful treatment often requires regular access to mental health care professionals and a variety of support services. Unfortunately, mental health care services are often not available or are under-utilized, particularly in developing countries. In developed countries, the treatment gap (the %age of individuals who need mental health care but do not receive treatment) ranges from 44% to 70%; in developing countries, the treatment gap can be as high as 90%. Common barriers to mental health care access include limited availability and affordability of mental health care services, insufficient mental health care policies, lack of education about mental illness, and stigma.
Limited Availability of Medication and Health Professionals
Unavailability of essential medicines is particularly prevalent in developing countries, and severely restricts access to treatment for psychological disorders. The World Health Organization reports that nearly 20% of countries do not have at least one common antidepressant, one antipsychotic, and one antiepileptic medication available in primary care settings. This problem is compounded by a lack of mental health care professionals in low- and middle-income countries; low-income countries have a median of 0.05 psychiatrists and 0.16 psychiatric nurses per 100,000 people. Even fewer resources are available for children and adolescents; the WHO reports that most low- and middle-income countries have only one child psychiatrist for every one to four million people in 2005. Community-based mental health care is also rare in low-income countries; about 52% of low-income countries offer community-based mental health care programs, compared to about 97% of high-income countries.
Limited Affordability
In many low- and middle-income countries, the high cost of psychiatric treatment, often due to high medication prices, poses significant financial barriers to patient care.(6) In addition, psychological disorders are not covered by insurance policies in many countries, making mental health care unaffordable for many people. The WHO also reports that 25% of all countries do not provide disability benefits to patients with mental disorders, and one-third of the world’s population lives in countries that allocate less than 1% of their health budget to mental health. Furthermore, 31% of countries do not have a specific public budget for mental health.
Policy Limitations
The World Health Organization cites a global lack of comprehensive mental health policies, which are crucial for implementing and coordinating mental health care services, as a key barrier to public access to mental health care. Nearly one-third of all countries, and almost half of all African nations, have no comprehensive mental health care policy or plan. Among countries with mental health care policies in place, approximately 40% have not been revised since 1990 and do not address recent developments in mental health care. Furthermore, 22% of countries do not have laws that offer legal protection of the human and civil rights of people with mental illnesses.(9) In many low- and middle-income countries, the localization of mental health care resources in large cities has also been cited as a key barrier to providing mental health care to the entire population, and geographical decentralization has been recommended to improve accessibility to mental health care in non-urban communities.
Lack of Education
In developing and developed countries, limited knowledge about mental illness can prevent individuals from recognizing mental illness and seeking treatment; poor understanding of mental illness also impairs families’ abilities to provide adequate care for mentally ill relatives. In 1992, data from the National Comorbidity Survey revealed that of the 6.2% of respondents who had a serious mental illness in the 12 months prior to the survey, fewer than 40% had received stable treatment. The majority of individuals with an untreated severe mental illness did not seek care because they believed they did not have a condition that required treatment. Of responders with a severe mental illness who did not receive care but recognized that they needed treatment, 52% reported situational barriers to care, 46% cited financial barriers, and 45% dropped out of care because they felt that treatment had not been effective. Furthermore, 72% of respondents who did not seek treatment chose to do so because they wanted to “solve the problem on their own”. These findings suggest that lack of education about the nature of psychological disorders and the need for consistent treatment is a significant barrier to care.
Stigma
Multiple studies have found that stigma associated with mental illness often prevents patients from seeking and adhering to treatment, as patients may “attempt to distance themselves from the labels that mark them for social exclusion”.
Priority Mental Health Conditions
The World Health Organization (WHO) identified several priority mental health conditions that “represented a high burden (in terms of mortality, morbidity, and disability); caused large economic costs; or were associated with violations of human rights”. The priority conditions are depression, schizophrenia and other psychotic disorders, suicide, epilepsy, dementia, substance use disorders, and mental disorders in children. The causes, symptoms, etiologies, and treatments of several of these priority disorders will be briefly discussed below.
Depression
Major depression is one of the most common mental illnesses, with a worldwide lifetime prevalence of approximately 12%. Symptoms of depression include sad mood, loss of interest in activities that used to be pleasurable, weight gain or loss , fatigue, inappropriate feelings of guilt, difficulty concentrating, and thoughts of suicide. Depression can cause problems at work, in personal relationships, and can lead to suicide . Depression rates are twice as high in women as in men. Depression has also been correlated with adverse health behaviors including smoking, alcohol abuse, physical inactivity, and sleep disturbances. Antidepressants are typically used to treat depression, as are psychotherapy and lifestyle changes. In treatment-resistant cases, some people turn to electroconvulsive therapy (ECT), in which the brain is electrically stimulated to reduce depressive symptoms. Psychotherapy or psychological counseling is often an important part of treatment, and includes improving problem-solving capabilities, setting goals, and changing depressive cycles of thinking. Lifestyle changes like regular exercise, avoidance of alcohol and drugs, and adequate sleep may lessen the effects of depression.
Schizophrenia
Although the lifetime risk for schizophrenia is only 0.08-0.44 %, the symptoms that characterize the disorder can severely impair daily functioning. Schizophrenia is a psychotic disorder categorized by a variety of symptoms. Positive symptoms (behaviors that are induced by the illness) include hallucinations ( perceiving stimuli that are not there), delusions (strongly held false beliefs ), thought disorders ), and movement disorders . Negative symptoms (the feelings or behaviors that are reduced or not present in those with the illness) include flat affect, loss of pleasure in daily life, and not speaking. Cognitive symptoms include a decreased ability to use information and make decisions, and problems with attention, focus, and working memory. Although schizophrenia is rarely cured, it can often be managed with antipsychotic medications and psychosocial interventions such as cognitive behavioral therapy . However, the nature of the disease, as well as the unpleasant side effects of the medications, often decrease patient adherence to treatment regimens.
Epilepsy
Epilepsy is characterized by repeated seizures caused by abnormal electrical signaling in the brain . Epilepsy is estimated to affect approximately 50 million people worldwide, or approximately 5-8 people per 1,000, of whom 80% live in developing countries. Epilepsy can be caused by stroke, dementia, congenital brain defects, brain injuries, some metabolism disorders, and tumors. Seizures can present differently depending on which areas of the brain are affected . Doctors in developed nations often diagnose epilepsy by monitoring the brain’s electrical activity using use EEGs (electroencephalograms) . Epilepsy treatment typically includes anticonvulsant medications or surgery, depending on the cause and severity of the seizures.
Dementia
Dementia is characterized by a loss of brain function that impairs memory, language, thoughts, judgment, and behavior. Dementia can be caused by stroke, brain tumors and other brain injuries, chronic alcohol abuse, and diseases such as multiple sclerosis, Parkinson’s disease, and Alzheimer’s disease (the most common type of dementia). Treatments for some forms of dementia include antipsychotics, mood stabilizers, and stimulants, though degenerative forms of dementia (such as Alzheimer’s disease) do not yet have a cure. As life expectancies increase worldwide, dementia is becoming an increasingly important global health issue. Currently, an estimated 24.3 million people worldwide have dementia, 60% of whom live in developing countries. By 2040, it is estimated that 71% of the projected 81.1 million dementia cases will be in the developing world.
Alcohol and Drug Abuse
The World Health Organization reports that 4.4% of the worldwide disease burden is attributable to alcohol consumption, and an estimated 200 million people worldwide used illicit drugs between 2005 and 2006. Studies suggest that alcohol and drug abuse in developing countries is rising due to urbanization, poverty, migration, changes in technology, lack of education, and the high profit potential associated with drug sales. Alcohol and tobacco each contribute 0.5 to 16% of the disease burden (DALYs) in developing counties. Excessive alcohol consumption can lead to injury, disease, and birth defects, while tobacco use increases the risk of a variety of cancers, and intravenous drug use contributes to the spread of HIV/AIDS. Substance abuse disorders are often addressed via prevention programs, psychological counseling, medication, and support groups.
Mental Disorders in Children
Common childhood mental disorders include autism, Down syndrome, fetal alcohol syndrome, and attention deficit disorder . Although the specific symptom set depends on the disorder, many developmental disorders are characterized by delayed achievement of (or failure to achieve) developmental milestones, limited cognitive functioning, impaired language or motor abilities, and behavioral problems. Childhood mental disorders are particularly challenging to address in low-income countries due to a lack of nutritional foods that aid in mental development, lower levels of parental education , and limited or no social services for developmentally-challenged children.
Causes of Psychological Disorders
Psychological disorders have etiologies that are largely multi-factorial, involving complex interactions between genetic and environmental factors. A number of risk factors have been implicated in the development of psychological disorders, but their relative contributions to mental illness are specific to different disorders and individual patients, and a precise cause can rarely be identified on an individual basis. Below is a sampling of some of the variables identified as risk factors in the development of psychological disorders.
Biological and Personal Factors
- Genetics
- Pathogens
- Injuries
- Problems during gestation or birth
- Substance abuse
- Cognitive style
Environmental Factors
- Poor nutrition
- Exposure to toxins
- Stressful life events
- Chronic stress
- Culture
- Abuse
- Poverty
- War
Gene by Environment Interactions: Schizophrenia and Depression
The factors listed above do not act in isolation to contribute to the development of psychological disorders, and the nature of gene by environment interactions is the subject of substantial research. Gene-environment interactions describe the phenomenon by which certain gene variants modulate the effects of environmental factors. However, environmental factors often cause epigenetic changes –chemical modifications that affect how genes are expressed – making it difficult to distinguish environmental from genetic effects. Increased interest in epigenetics has prompted modern psychiatric research to focus on biochemical mechanisms by which environmental factors may influence genetic expression and the onset of psychological disorders. The following studies illustrate the complex nature of gene by environment interactions by providing a sample of research on the causes of schizophrenia and depression, two of the priority mental health conditions identified by the World Health Organization.
Schizophrenia
Schizophrenia has long been believed to have a strong genetic component. Twin studies report the concordance rate of schizophrenia (the probability that one twin will have the disorder if the other twin does) to be 45 to 60 % for monozygotic (identical) twins, compared to only 10 to 15 % for dizygotic (fraternal) twins. In a comprehensive review of schizophrenia literature, Husted et al. (2012) emphasize that many studies have also identified a host of environmental risk factors for schizophrenia. For instance, a classic study of the Dutch Hunger Winter (1944-1945) found that exposure to famine early in pregnancy was associated with a significant increase in schizophrenia risk for both male and female offspring. However, because of the retrospective nature of the study, researchers could not determine which of the many variables associated with famine (e.g. nutrient deficiencies, generalized stress, infection, ingestion of toxic substances, or a combination of those factors) contributed to the increased risk of psychosis. Determining the relative contribution of environmental factors to the onset of schizophrenia is further complicated by the interactions between genetic and environmental variables. For instance, Caspi et al. (2005) found that different versions of the catecholamine-O-methyl transferase (COMT) gene, which is involved in the regulation of dopamine release in the prefrontal cortex, affected the degree to which adolescent cannabis use was a risk factor for schizophrenia.
Depression
The genetic contribution to depressive disorders is estimated to be approximately 30 to 40 %. While a variety of environmental characteristics have been identified as risk factors for depression, early life stressors, such as childhood physical or sexual abuse, parental neglect, and loss of a parent, have been shown to significantly increase the probability of developing depression later in life. The effects of early life stressors are influenced by a variety of genes, and the 5-HTTLPR gene, involved in serotonin transporter functioning, has received significant attention. Caspi et al. (2003) found that the short version of the gene, which is associated with a reduction in serotonin transporter function, increased the risk of developing depressive symptoms and suicidality following exposure to stressful life events and maltreatment during childhood. However, results from studies of the 5-HTTLPR gene have not been consistent, and Heim et al. (2012) suggest that such variation occurs because different genetic backgrounds may alter the nature of the 5-HTTLPR gene by environmental interaction. Furthermore, a variety of other genes may influence this interaction, as a number of gene-environment interactions have been reported in recent studies of the 5-HTTLPR gene.
Improving Mental Health Care
Goals, Strategies, and Considerations
The World Health Organization (WHO) recommends an “optimal mix of services pyramid”, in which mental health care services that cost the least and are the most frequently needed (e.g. self-care and informal community care) form the base of the pyramid, while more expensive services needed by a smaller fraction of the mentally ill population (e.g. long-term inpatient care facilities) are at the top of the pyramid. To develop this mix of services, the WHO recommends that countries:
- Limit the number of mental hospitals
- Build community mental health services
- Develop mental health services in general hospitals
- Integrate mental health services into primary health care
- Build informal community mental health services
- Promote self-care
Through its Mental Health Global Action Programme (mhGAP), the WHO has proposed multiple strategies to improve mental health care delivery. The four core strategies listed by the mhGAP are:
- Increasing and improving information for decision-making and technology transfer to increase country capacity.
- Raising awareness about mental disorders through education and advocacy for more respect of human rights and less stigma.
- Assisting countries in designing policies and developing comprehensive and effective mental health services.
- Building local capacity for public mental health research in poor countries.
Implementing the WHO’s recommendations will require investment by the global health community, including governments, donors, multilateral agencies, and consumer groups. Chisholm et al. (2007) investigated the level of investment required to scale up mental health care in 12 countries for which data from the WHO-Assessment Instrument for Mental Health Systems (AIMS) were available. The countries studied included four low-income countries (Ethiopia, Nepal, Nigeria, and Vietnam), seven lower middle-income countries (Albania, China [Hunan province], Iran, Morocco, Paraguay, Thailand, and Ukraine), and one upper middle-income level country (Chile). The researchers chose targets for improvement based upon levels of service coverage for mental illness achieved in high-income countries; targets were set at 80% improvement in coverage of services for people with schizophrenia and bipolar affective disorder, 25% improvement in coverage for hazardous alcohol use services, and 33% improvement for coverage of services for depression. To reach these targets within ten years, total expenditures in the low-income countries would need to rise ten-fold, to about $2 per person per year by 2015, and total expenditure in the lower middle-income countries would need to increase between three-fold and six-fold, to about $3-4 per person per year. This would likely require an “initial period of large-scale investment”, a $0.30-0.50 per person per year spending increase, followed by a gradual increase in spending of about $0.10-0.25 per person per year. Although this model does not include targets for scaling up services for childhood mental disorders, and is based on data from a small sample of countries, it can be adapted by other countries to guide investment in mental health care services.
Chisholm et al. (2007) emphasize that mental health indicators must be carefully selected to monitor the scaling-up process, to ensure that countries can measure their progress and compare their mental health care status to that of other countries. Chisholm et al. (2007) offer a set of 11 indicators to quantify progress towards four recommended mental health goals:
- Sufficient planning and investment for mental health care
- Sufficient workforce to provide mental health services
- Consistency of mental health care inputs and processes with best practice and human-rights protection
- Improved outcomes for people with mental disorders
In addition, the scaling-up process must be accompanied by research funding to investigate the efficiency and effectiveness of treatment and prevention interventions for mental illness. In particular, Chisholm et al. (2007) argue that funding should be concentrated on research efforts to “develop and assess interventions for people with mental disorders that do not need to be delivered by mental health professionals, and to assess how health systems can scale up such feasible and effective interventions across all routine-care settings”. One strategy to scale up mental health interventions in routine-care settings is to integrate mental health care into primary care services. Incorporating aspects of mental health care into the primary care setting is expected to provide a more holistic approach to health care, enable earlier detection and treatment of mental illness, increase ease of access to mental health care, and reduce the stigma associated with seeking psychiatric care. In order to ensure effective and high-quality mental health services, the integration of mental health care into primary care services must be accompanied by adequate resources and specialized education and training for primary health care professionals.
While the WHO’s recommendations for scaling up health care offer a general set of strategies for improvement, nations should implement culturally sensitive strategies for optimal mental health care delivery. For instance, in Japan, where deinstitutionalization began in the mid-2000s, family members have historically played a central role in providing care for relatives with severe mental illness. Due to the extensive involvement of family members in mental health care, assertive community treatment (ACT) has been recommended as an essential component of improving mental health care in Japan. This is partially because ACT provides comprehensive mental health care to patients, thereby lightening the burden of care on families, while allowing family members to remain involved in the care of their relatives.
In conclusion, to improve global access to mental health care, the scaling up of mental health care services must be closely monitored, sensitive to cultural context, accompanied by extensive research, and supported by adequate funding.
After the Asylum: How America’s Trying to Fix Its Broken Mental Health System
Patients with mental illness are being detained in emergency rooms, often for weeks at a time. Now some states are rethinking the entire psychiatric care system.
Patients with mental illness are being detained in emergency rooms, often for weeks at a time. Now some states are rethinking the entire psychiatric care system.A couple of years ago, in Pierce County, Wash., 10 mental patients spent extended periods in hospital emergency rooms after suffering psychotic episodes. This was against the rules: Washington state law requires that such patients see a psychiatrist and then move to a mental health facility or psychiatric unit within a larger hospital. But in each case, the hospital staff simply couldn’t find a place that had any room. So the patients stayed in the ER — some for as long as two weeks.
This practice is called psychiatric boarding, and it happens all over the country. It’s often the only option for emergency room staff; they can’t turn away mentally ill patients, even though they’re not trained to deal with them. Essentially, all they can do is stabilize the patients and keep them in bed, often in seclusion or strapped down for days or weeks at a time.
Psychiatric boarding is an ugly reality that patients and physicians reluctantly accept. But that wasn’t the case with the 10 patients in Pierce County. Their families sued the state.
Last year, the Pierce County case made its way up to the Washington state Supreme Court, where the justices ruled unanimously that psychiatric boarding was unlawful. Washington is still the only state with a law banning the practice, but in the wake of the court decision a surprisingly diverse coalition of physicians, mental health advocates and government health-care officials have begun calling for solutions to boarding. They say the practice is unethical and warrants a nationwide effort to provide more humane and medically effective alternatives to long, unnecessary ER stays. “Evidence all around us demonstrates the mental health care system is in crisis,” said Dr. LaMarr Edgerson, director-at-large of the American Mental Health Counselors Association, at a U.S. House committee hearing last year. The broken system, Edgerson explained, “is generating increased demand for inpatient psychiatric beds while simultaneously decreasing their supply.”
What the Pierce County patients experienced is the rule, not the exception. In a survey last year, the American College of Emergency Physicians found that 84 percent of emergency rooms said they board psychiatric patients, and it’s getting worse. More than 50 percent said they spend increasing time and energy trying to transfer those patients to appropriate psychiatric facilities.
In Washington state, emergency room physicians joined an amicus brief in support of the Pierce County patients, agreeing that psychiatric boarding resembled warehousing more than it did medical care. They painted a picture of hurried, chaotic emergency rooms that were adding to the patients’ agitation and anxiety. The physicians laid blame on the Washington Legislature, which cut mental health funding by more than $90 million between 2009 and 2012.
Physicians don’t want psychiatric patients waiting for weeks in the emergency room, and they’re searching for other options, says Stephen Anderson, who lives in Pierce County and sits on the board of directors of the American College of Emergency Physicians. So far, no court outside Washington state has weighed in on the issue, but emergency room physicians in half a dozen states have invited Anderson to talk to them about the Pierce County case. “Everybody is looking at it and saying, ‘Do we need to get to this point?’” Anderson says. “I don’t know a colleague anywhere in the nation who doesn’t have psychiatric boarding in their ER.”
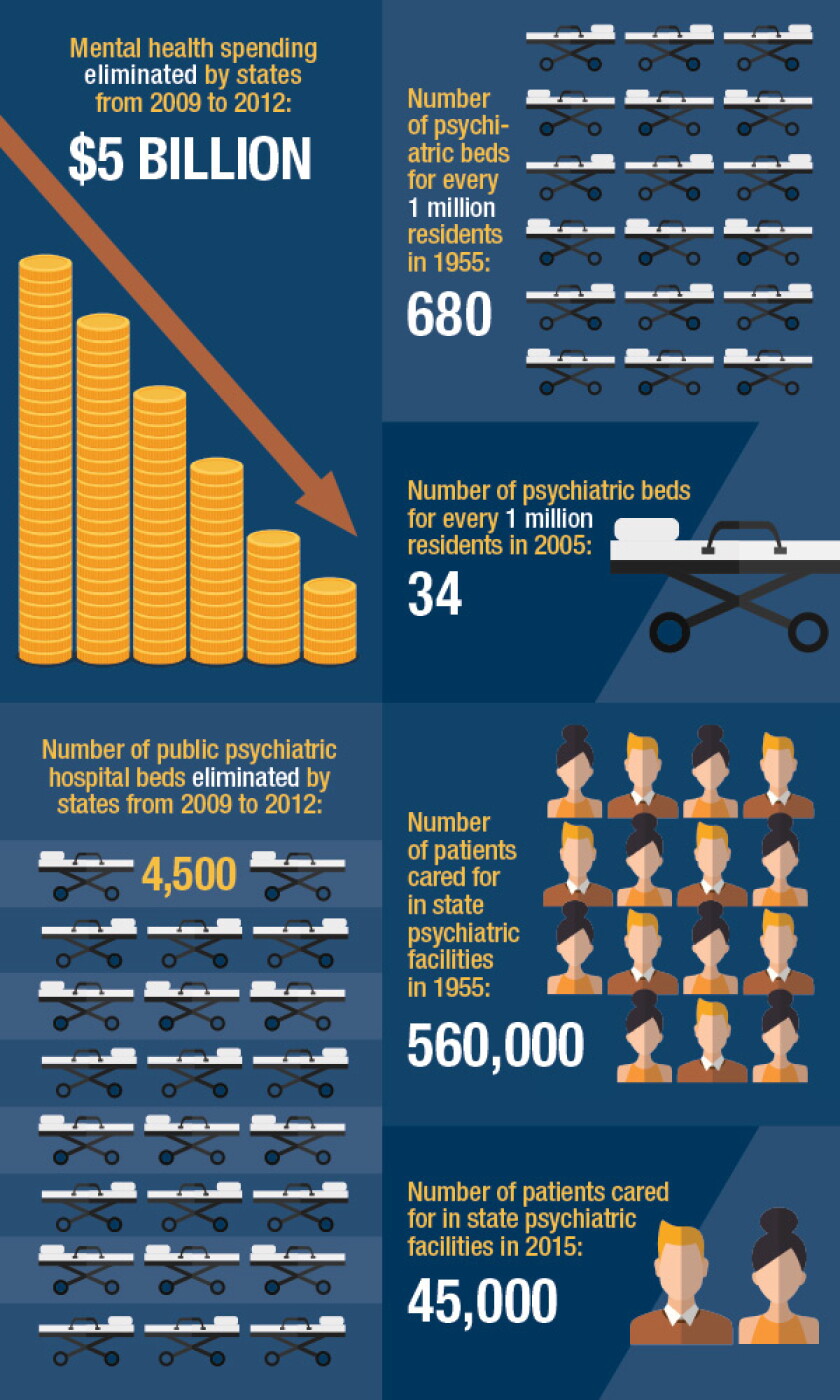
The fundamental reason boarding occurs is that there are more people with severe mental illness than there are psychiatric beds to house them. The gap is widening. Over a period of 50 years, starting in the mid-1950s, the per capita number of such beds in the United States decreased by 95 percent, from 680 beds per million residents in 1955 to 34 per million in 2005. Much of that decline is due to the closing of state asylums. In 1955, state psychiatric facilities cared for 560,000 patients. Today, they care for 45,000.
The number of psychiatric beds in America has declined 95% since the mid-1950s.
The bed shortage is also the result of a provision in the 1965 federal Medicaid law that allows Medicaid reimbursements for psychiatric care only in small facilities. Up until that law took effect, states bore the responsibility of paying for psychiatric care, usually offered at large public mental hospitals. But those hospitals had earned a negative reputation as poorly maintained warehouses that made patients worse. So the law excluded psychiatric hospitals with more than 16 beds. The expectation was that smaller community-based facilities would take over much of the job of mental health treatment, and that these would be able to tap into Medicaid funding.
The exclusion of funds for large mental institutions was a political victory for a bipartisan coalition of fiscal conservatives who wanted to cut mental health spending and liberals who saw state hospitals as sites of human rights abuses. But the exclusion had an unintended consequence. For the first time, states could collect partial reimbursements from the federal government for psychiatric care as long as they shifted treatment away from the old public mental hospitals. What followed was the natural consequence of that financial incentive: a national movement not just to de-emphasize large state psychiatric hospitals but to close them altogether, a process better known today as deinstitutionalization.
The theory was that fewer patients would need the state hospitals because of advances in psychotropic drugs that could stabilize their conditions; any care they still required could be met by the smaller outpatient clinics and other community-based facilities. But very few of these smaller facilities were actually created. When states closed the older hospitals, they simply cut back mental health funding rather than switching to the new model. The minimum ratio of psychiatric beds to patients should be about 50 beds per 100,000 residents, according to the Treatment Advocacy Center, a national nonprofit dedicated to helping patients with severe mental illness. No state meets that standard.
Today, because there aren’t enough beds, a majority of the nation’s mentally ill end up homeless, incarcerated or as chronic visitors to emergency rooms. An estimated 16 percent of the prisoners in jails and state prisons have a serious mental illness. Anyone who has such an illness is about three times more likely to be in a jail or in a state prison than in a psychiatric facility. That’s why the Treatment Advocacy Center calls deinstitutionalization “the greatest social disaster of the 20th century.”
Federal health officials have been trying to undo some of the damage that the defunding of large mental hospitals has caused. In fact, a section of the Affordable Care Act calls for research to see what would happen if Medicaid went back to reimbursing these institutions for treating patients. In 2012, 11 states and the District of Columbia agreed to participate in a demonstration project to test whether a change in the Medicaid payment model would result in better access to psychiatric care while also lowering Medicaid costs. If the demonstration worked as proposed, mentally ill patients would spend less time in emergency rooms and psychiatric boarding might begin to fade away.
Both state Medicaid officials and their federal counterparts have reason to believe the experiment will be a success. In Maryland, for example, the Department of Health and Mental Hygiene reported that the daily cost of care for a mental patient at an acute care hospital is $2,965. At a private psychiatric facility, the cost is $864. “Not only do we know that it is cost-effective, but we know that this is what they do: It’s their specialty,” says Shannon McMahon, Maryland’s deputy secretary of health-care financing. While a general hospital might have staff with behavioral health expertise, she says, “you want to go to the place that does it the most — a center of excellence.”
Up until now, in many states, these centers of excellence have primarily been available to people with private health insurance through their employer. Thus, the demonstration is also testing what would happen if low-income patients covered by public health insurance had better access to private facilities that specialize in psychiatric care. Would their health outcomes be better? Would they spend less time in emergency rooms? Medicaid patients have a right to find out, says Andrew Sperling, director of federal affairs for the National Alliance on Mental Illness. “We ought not to say that just because you’re on Medicaid and poor, you can’t go to those places.”
The demonstration finished last summer, but a third-party evaluation by Mathematica Policy Research, a private contractor, won’t be completed until September of next year. That didn’t stop U.S. Sen. Ben Cardin of Maryland from ushering a bill through the Senate that would extend the project for an additional year and expand it to large public psychiatric facilities in the 11 states, so long as it didn’t increase net spending in the overall Medicaid program. (The Congressional Budget Office scored the bill as costing $100,000 in direct spending over the next 10 years.) As of November, a companion bill in the House was in committee but hadn’t received a hearing.
A parallel effort with similar goals is also garnering attention. Earlier this year, the Centers for Medicare and Medicaid Services released a proposed rule that would affect more private hospitals and could open access to more beds. The rule would grant a waiver for large private psychiatric facilities to receive Medicaid managed care payments for short-term stays of less than 15 days. Unlike the demonstration, it would apply nationwide.
But the demonstration project and the federal waiver in no way constitute a solution to the problem. Under the demonstration, Medicaid reimbursements are available to only a subset of patients with serious mental illness: adults between the ages of 21 and 65 who have expressed suicidal or homicidal thoughts or gestures, or patients deemed dangerous to themselves or others. In its interim report, Mathematica notes that children under 21, adults older than 65 and patients with many common mental illnesses, such as schizophrenia, don’t qualify.
The same interim report notes that the average length of stay for a patient was 8.2 days. At first blush, that seems like good news, since it suggests that making Medicaid payments available for 15-day stays would cover the average patient. But the demonstration only looked at a narrow subset of potential patients. Other data suggest the median length of stay for all psychiatric patients well exceeds 30 days. Even with high-quality specialty care, many aren’t ready to return to the community in two weeks.
And even if the federal government unlocked Medicaid as an insurer for private psychiatric care, the overall system would still have far too few beds to meet demand. The Treatment Advocacy Center estimates that to reach a minimum level of psychiatric care, as many as 95,000 new beds would be necessary.
Given all these problems, some health-care advocates have proposed a remedy that would have been unthinkable just a few years ago: returning to the traditional mental hospital, the very institution that reformers fought so hard to abolish in the 1960s. Last January, Dominic Sisti and two co-authors from the University of Pennsylvania medical school called for the return of long-term psychiatric care in a journal article titled, “Bring Back the Asylum.” They wrote that “for persons with severe and treatment-resistant psychotic disorders, who are too unstable or unsafe for community-based treatment, the choice is between the prison-homelessness-acute hospitalization-prison cycle or long-term psychiatric institutionalization.” They left no doubt that they considered institutionalization to be the best option.
Shortly after the article ran, Sisti says, “I was deluged with cranky and almost angry emails.” Some critics accused him of advocating a return to the inhumane treatments and overcrowded conditions portrayed in Ken Kesey’s famous book, One Flew Over the Cuckoo’s Nest. Sisti and his co-authors responded that they were asking readers to imagine a new type of institution, one that would be a safe and caring refuge for mentally ill patients who were unsuited for community-based care. They wouldn’t be the asylums of the 1950s and wouldn’t have to be called asylums, despite the perhaps unfortunate title of the article. “We have this hole in our spectrum of health care for mentally ill individuals,” Sisti says. “We were looking to inject ourselves into the conversation.”

The Washington state Supreme Court ruled last year that psychiatric boarding is unlawful. (Flickr/Harvey Barrison)
Last year, when the Washington Supreme Court ruled that psychiatric boarding was unlawful, it didn’t spell out a remedy. In practice, that meant people could still end up in the emergency room during a psychotic episode. The court directed that hospitals have a psychiatrist available to screen the patients and then return every day to make evaluations and prescribe medication. “It was not an unreasonable thing to have asked for,” says Anderson, the emergency room physician in Pierce County. But smaller general hospitals don’t have the personnel to comply with the decision. As Anderson puts it, “you had to turn them loose after 72 hours, or you had to hope that nobody was going to arrest you.”
The court put a four-month stay on its ruling, giving Gov. Jay Inslee and the legislature time to make changes that would relieve some of the pressure on emergency rooms. He found $30 million for new mental health funding, and he prevented the elimination of almost 40 state psychiatric beds across the state. Inslee also converted 140 psychiatric beds previously set aside for voluntary-commitment patients and repurposed them for patients committed involuntarily.
In addition, the legislature passed a law this year that allows emergency rooms to use telepsychiatry to conduct an initial patient evaluation. Staff bring a screen to the patient’s bed and a psychiatrist consults remotely. Because the consultation is taking place in an emergency room, not a large psychiatric facility, Medicaid pays for it.
Telemedicine is a modest fix for some of the smaller general hospitals in rural and small-town Washington, where too few psychiatrists are available to work in emergency rooms. With telemedicine, a psychiatrist anywhere in the country can reach an initial diagnosis, prescribe medication and help the emergency room physicians decide whether the patient requires long-term psychiatric care somewhere else, or can return to the community in a few days.
But the mental health system in Washington doesn’t just need psychiatrists, it needs beds, and they will remain hard to come by for the foreseeable future, despite the court decision and its aftermath. “The state moved it from the back burner to the front burner and it has helped us,” Anderson says. “It’s a whole lot further than we were two years ago, but the need for inpatient psychiatric care is not going away.”
The Top Issues Facing Mental Health Care
Approximately 1 in 5 Americans ages 18 or older lives with a mental illness. Issues facing mental health care delivery are only exacerbating the problem.
Successful treatment of these conditions requires regular access to mental health care professionals and various support services – things so many Americans and Canadians don’t have easy or guaranteed access to.
It’s why the barriers to mental health care are among the most significant issues for people seeking treatment.
In this article, we explore the three biggest reasons why people are deterred from accessing mental health. Then we look at howvirtual carehas the potential to eliminate these issues facing mental health care.
Importance of Overcoming Challenges to Mental Health Treatment
Removing the barriers to mental health treatment is essential for improving lives and communities.
Nearly 800,000 people commit suicide every year, which is an average of 1 person every 40 seconds taking their own life.
With the proper treatment to address mental health conditions, we can reduce:
- Suicide rates
- Legal issues
- Family conflict
- Employment issues
- Substance abuse
- Physical health problems
But, to improve the mental health care framework, we’ll first have to understand barriers to mental health services that stop people from getting the care they need.
Biggest Barriers to Mental Health Care Access

- Financial Barriers
Financial barriers are among the top challenges in mental health services that hinder people from receiving needed care. People often cite concerns about the cost of care or lack of health insurance coverage when forgoing treatment.
In the National Comorbidity Study, 47 percent of respondents with a mood, anxiety, or substance use disorder said they thought they needed mental health care but couldn’t afford to get help.
How Can Virtual Care Reduce Wait Times?
Virtual care can make mental health treatment more affordable by reducing barriers to mental health care, such as:
- Taking time off work
- Transportation costs
- Finding child care
A program in the United States found that replacing nurse home visits with videoconferencing more than doubled their caseload capacity. Over 14 months, 43,560 driving minutes were saved.
In British Columbia, the Northern Health authority saved C$65,520 ($49,584.14) in annual travel costs alone by replacing in-person visits with telehealth sessions.
- Wait Times
Another of the major problems with the mental health system is long wait times. The longer the wait, the poorer the patient’s mental and physical health, and the less interested they are in seeking treatment.
A recent Children’s Mental Health Ontario (CMHO) study found that, in some communities, children may have to wait as long as two-and-a-half years to receive mental health treatment.
As for adults, psychiatrists see them based on priority or urgency. Despite that, they may be waiting for up to two weeks to be seen for psychoses, severe mood disorders, or an episode of mania.
How Can Virtual Care Reduce Wait Times?
Virtual care can provide direct interventions and real-time interaction between therapist and patient (for instance, videoconferencing). Other digital mental health interventions, which can complement therapy, include:
- Online mental health surveys
- Telephone-based hotlines
- Online access to mental health educational materials and resources
- Accessibility
Lack of access to mental health care can mean different things to different people.
For instance, older or less mobile patients may not have family or friends who can provide care and take them to clinics. In rural and low-income communities there can be a significant shortage of mental health providers and services.
Other factors that limit access include:
- Lack of transportation
- Social stigma
- Insufficient information
- Inadequate bandwidth and internet
How Can Virtual Care Improve Access to Mental Health Treatment?
Up to 80% of clinically stable patients can be treated through teleconsultation as their only point of contact. That means most people can video conference with a psychiatrist or therapist from the comfort of their own homes and still receive the full benefit of the treatment.
Removing Barriers to Mental Health Services With Virtual Care
Virtual care can successfully address some of the biggest problems with the mental health system and reduce the burden of providing treatment.
It’s time to use the best features of these technologies to start motivating patients and to build a more responsive and efficient health care system to address the problems with mental health care today.
So how do physicians motivate patients to approach them for mental health care online? There are many benefits for patients seeing physicians virtually compared to office visits, including:
- Treatments can be accessed anywhere at any time
- Little-to-no waiting lists/wait times
- Real-time communication with the physician
- Reduced disruption to work and personal schedules
- Not having to travel or arrange transportation
- Freedom to speak with the physician from the privacy of their own home
Conclusion
I am sure that unless you live in a cave or a monastery you have heard of serial killers and of mass shootings and other heinous crimes like these. You have to ask yourself what type of person would do these things? The answer would be mentally deranged individuals that is who. There just cannot be any other answer for it. So why do we have so many individuals like this running around our county-side? They seem to be acting with impunity. The answer is that we dropped the ball. We have let them down either in the way they were raised or educated or in the lack of help that they have received. One of the roadblocks is that there is a stigma placed on mentally handicapped people. Also quality psychiatric help does not come cheap. For one, there are few psychiatrists available. I am an RN, and I have taken care of many legal hold 2000 or L2K patients, and the wait is usually longer than the 72 hours before they can be seen at our hospitals. What eventually happens is that they are seen by trained social care workers. However, these individuals just don’t have the training to truly evaluate complicated cases. This is how a lot of sick individuals just slip through the system. Our Veterans Administration is also to blame. We train our soldiers to kill when they are ordered. They are given all the tools to be effective at their jobs, they are however not told how to deal with all the blood that is on their hands when they are discharged. When they are discharged they are pretty much left to their own devices. If they develop issues, it may be too late by the time they receive help. Our veterans have the highest suicide rates among any subgroups in the US.
The reason we have these extreme crimes is because our mental health care system is broken. Now that we know what the problem is, we have to fix it. We need more highly trained individuals to care for these people. We also need to financially compensate them as well. If we stopped helping everybody else in the world and took care of our own problems we would have the resources to take care of our problems. Stop messing around with the green new deal and all the hair brained programs we have and let the people take care of their own business. The economy will fix itself if big brother just gets the hell out of the way. I am frankly tired of having well over a third of my income pissed away with no measurable results.
Resources
governing.com, “After the Asylum: How America’s Trying to Fix Its Broken Mental Health System; Patients with mental illness are being detained in emergency rooms, often for weeks at a time. Now some states are rethinking the entire psychiatric care system.” By J.B. Wogan; adracare.com, “The Top Issues Facing Mental Health Care.” By The Adracare Team; uniteforsight.org, “A Brief History of Mental Illness and the U.S. Mental Health Care System.”; origins.osu.edu, “America’s Long-Suffering Mental Health System.” By Zeb Larson;
Addendum
America’s Long-Suffering Mental Health System
Afamiliar scene plays out again and again in American public life in the 21st century. In the wake of a mass shooting such as the one in Parkland, FL, commentators, pundits, and politicians all gather around to talk about the country’s broken mental health system and suggest its connection to the violence.

Nikolas Cruz—the suspected gunman at Marjory Stoneman Douglas High School in Parkland, FL—being arrested (left). A graph depicting mass shooting deaths in the U.S. from 1982 to 2016 (right).
{kind=link}
{kind=link}
Their solutions, however, are few to none. Whether Nikolas Cruz’s mental illness was a factor in the shooting is still being investigated, but the ease with which we talk about a defective mental health system is juxtaposed with a paucity of concrete solutions.
This pattern raises the question of whether the American mental health care system is in fact broken. The metrics we have don’t paint an encouraging picture.
The U.S. Department of Health and Human Services reports that one in five Americans has experienced issues with mental health; and one in ten youth have suffered a major bought of depression.

A vigil for increasing mental health care at Cook County Jail in 2014 (photo credit: Sarah-Ji).
The effects of mental illness on life quality of life and health outcomes are significant. Individuals with severe mental illness such as schizophrenia, major depressive disorder, or bipolar disorder (about four percent of the population) live on average 25 years less than other Americans. As many as a third of individuals with a serious diagnosis do not receive any consistent treatment.
The mentally ill are far more likely to be the victims of violent crime rather than the perpetrators. Only 3-5% of violent crimes can be tied in some way to a person’s mental illness, and people with mental illnesses are ten times more likely to be the victims of violence than the general public.
And while the relationship between mental illness and poverty is complicated, having a severe mental illness increases the likelihood of living in poverty. According to some estimates, a quarter of homeless Americans are seriously mentally ill.

Darren Rainey, who suffered from schizophrenia, died in 2012 from burns to over ninety percent of his body after prison guards locked him in a shower for two hours with 180°F water (left). A graph and chart showing the percentage of inmates with and without mental health problems in state prisons in 2006 (right).
{kind=link}
Most troubling, perhaps, is the criminalization of mental illness in the United States. At least a fifth of all prisoners in the United States have a mental illness of some kind, and between 25 and 40 percent of mentally ill people will be incarcerated at some point in their lives.
A study by Human Rights Watch revealed that prison guards routinely abuse mentally ill prisoners. Darren Rainey, a mentally ill prisoner at the Dade Correctional Institution in Florida, was boiled to death in a shower after being locked in it for more than two hours by prison guards.
More are sent to prison in part because fewer mental health facilities are available. The disappearance of psychiatric hospitals and asylums is part of the long-term trend toward “deinstitutionalization.” But jails and prisons have taken their place. Today, the largest mental health facilities in the United States are the Cook County Jail, the Los Angeles County Jail, and Rikers Island.

The entrance to Cook County Jail in Chicago, IL (left). The Angeles County Jail in downtown Los Angeles, CA (center). An areal view of the Rikers Island prison complex in New York City (right).
{kind=link}
{kind=link}
So how did we get to the point where mental illness is frequently untreated or criminalized?
Activists, advocates, and professionals like to pin the blame on Ronald Reagan, particularly his 1981 Omnibus Budget Reconciliation Bill, which raised defense spending while slashing domestic programs. One of the cuts was to federal funding for state community mental health centers (CMHCs).

President Ronald Reagan outlining his tax plan in a televised address from the Oval Office in 1981.
{kind=link}
However, attributing the present state of the system solely to Reagan would ignore the prevailing patterns in mental health care that came before him. Three impulses have long shaped the American approach to mental health treatment.
One is an optimistic belief in quick fixes for mental illness to obviate long-term care, ranging from psychotropic medications to eugenics. The second is a more pessimistic determination to make the system work as cheaply as possible, often by deferring the costs to somebody else and keeping them from public view. Last is the assumption that people with mental illnesses are undeserving of charity, either because of genetic defects or because they should be curable and thus not under long-term care.
Indeed, mental health care occupies a paradoxical place in the history of social welfare in the United States, where aid is socially accepted only for the “deserving needy.” People with mental illnesses rarely fit this mold. At times, behaviors deemed socially aberrant were classified as mental illness (the American Psychiatric Association designated homosexuality a mental illness until 1973).

The Birth of the Asylum and the Hospital
The nineteenth century saw the growth of something like an organized asylum system in the United States. Asylums themselves were nothing new. London’s Bethlem Royal Psychiatric Hospital, better known as Bedlam, was founded in 1247. In the United States however, the creation of these asylums took time, in part because their cost was deferred to state governments, which were leery of accepting the financial burden of these institutions. Consequently, local jails often housed ill individuals where no local alternative was available.

An engraving of Bethlem Royal Psychiatric Hospital in London, England around 1750.
_at_Moorfields,_London_Wellcome_V0013175.jpg){kind=link}
Early in the 19th century, patients in asylums were called “acute” cases, whose symptoms had appeared suddenly and whom doctors hoped to be able to cure. Patients who were deemed “chronic” sufferers were cared for in their home communities.
The so-called chronic patients encompassed a wide range of people: those suffering from the advanced stages of neurosyphilis, people with epilepsy, dementia, Alzheimer’s disease, and even alcoholism.
The number of elderly patients in need of assistance and treatment increased in tandem with increasing lifespans during the 19th century. As county institutions grew crowded, officials transferred as many patients as they could over to new, state-run institutions in order to lower their own financial burdens.

Oregon State Hospital for the Insane opened in 1883 and is one of the oldest continuously operated hospitals on the West Coast (top left). Oregon State Hospital was both the setting for the novel (1962) and the filming location (1975) of Ken Kesey’s One Flew Over the Cuckoo’s Nest (top right). The patient population at Eastern Oregon State Hospital tripled in its first fifteen years (bottom left). Built to relieve the overcrowding at Oregon State Hospital, Eastern Oregon State Hospital in Pendleton itself quickly became overpopulated (bottom right).
{kind=link}
#/media/File:One_Flew_Over_the_Cuckoo%27s_Nest_poster.jpg){kind=link}
Oregon State Hospital’s story is typical. It housed a population of 412 in 1880, expanded to nearly 1,200 by 1898, and in 1913 opened a second state hospital to house a patient population that had more than quadrupled since 1880.
Most other states confronted similar circumstances. Some built a host of smaller institutions in different counties while others concentrated their populations in a few large institutions. But the end result was the same: hospitals proliferated and grew bigger. New York’s inpatient population (which, to be sure, had outsized proportions) was 33,124 in 1915; by 1930, it was 47,775.

As the institutionalized population mushroomed, treatment of the mentally ill evolved. Doctors throughout the 19th century placed their hopes in what was they called “moral treatment,” rehabilitation through exposure to “normal” habits. In many cases, these habits included working. Most institutions were attached to farms, partly to provide food for the people living there, but also to provide “restorative” work. Others had workshops.
There is, at best, mixed evidence on whether such treatments were effective, although supporters claimed high rates of recovery for patients treated in asylums. In any event, moral treatment was only ever intended for acute cases, so it fell out of fashion under pressure from the ever-multiplying population in hospitals.

Patients performed manual tasks like shoe-making at the Willard Asylum for the Insane in New York (left). Female patients engaged in agricultural labor at a mental health facility (right).
Combined with changing patient demographics, hospitals were increasingly serving as custodial institutions. Doctors working with patients suffering from dementia or late-stage neurosyphilis could not expect those in their care to improve. The role of medical professionals shifted from therapy to caretaking.
Prevention: Eugenics as a “Cure” for Mental Illness
Discontented with the idea of being mere caretakers, psychiatrists began to work toward cures and preventive techniques in the late 19th and early 20th centuries. The most conspicuous manifestation was the growth of eugenics and forced sterilization. These “cures” targeted specific populations, such as immigrants, people of color, the poor, unmarried mothers, and the disabled.

Southern asylums in the Jim Crow era were segregated and ones for African Americans received far less funding and accordingly suffered from chronic overcrowding, abuse, and generally deplorable conditions. An investigative commission in 1909 found Montevue Asylum in Maryland to be one of the state’s worst facilities. Patients there slept on floors with minimal bedding (left), were often shackled (center), and had little space during the day (right).
Although expressing some reservations about who was receiving eugenic treatment, many psychiatrists enthusiastically supported it. While doctors remained skeptical about the possibility of curing people with severe and persistent mental illness, preventing it through eugenics promised to solve the problem for future generations.
In 1896, Connecticut became the first state to prohibit marriage for epileptics, imbeciles, and the feeble-minded. In 1907, it was also first to mandate the sterilization of an individual after a board of experts recommended it. Thirty-three states ultimately adopted sterilization statutes, though certain states carried out a disproportionate number of these, with California alone accounting for a third of such operations. Ultimately, more than 65,000 mentally ill people were sterilized.

A 1929 map of states that had implemented sterilization legislation (left). Carrie Buck and her mother Emma Buck at the Virginia Colony for Epileptics and Feebleminded in 1924 (right). Emma had been committed after accusations of immorality, prostitution, and having syphilis. Her daughter was committed after becoming pregnant at seventeen as the result of a rape.
{kind=link}
While we now know that these sterilizations did not prevent mental illness, courts supported the programs. In Buck v Bell, Supreme Court Justice Oliver Wendell Holmes, Jr. argued that sterilizations did not violate people’s rights, concluding “three generations of imbeciles is enough.”
After World War II, revelations about Nazi war crimes turned many citizens against such procedures, but the procedures persisted in some places well into the late twentieth century, disproportionately affecting racial minorities. In Oregon, for example, the Board of Social Protection performed its last surgical sterilization in 1981 and disbanded two years later.

A protest against forced sterilizations in North Carolina around 1971 (left). A historical marker in Raleigh, NC regarding the 7,600 people sterilized in that state (right).
From Prevention to Treatment
Beginning in the early 20th century, some doctors wanted to try new treatments for mental illness rather than preventive measures. They focused on the body instead of lifestyle or psyche. In trying to find physiological origins for maladies, psychiatrists hoped they might treat schizophrenia, manic depression, and other illnesses.
Electroconvulsive therapy (ECT), which induces seizures in people through a series of electrical shocks, became one of the most famous such treatments and is still in limited use today. ECT remains controversial, not least because of its use on non-consenting individuals and its side effects.

Electroconvulsive therapy being administered at a Liverpool, England facility in 1957.
.jpg){kind=link}
But clinical data indicates it can be effective in mitigating or eliminating symptoms for long periods of time. The same cannot be said for other treatments for schizophrenia and bipolar disorder that emerged in the 1920s.
Building off of the success of malaria therapy in curing syphilis (which involved deliberately exposing patients to malaria), the Austrian therapist Manfred Sakel introduced insulin shock therapy in 1927 as a cure for schizophrenia. He injected patients with successively larger doses of insulin, often to the point of inducing a coma, then revived them with glucose and repeated the procedure. The more fortunate patients emerged from this with considerable weight gain; the less lucky with permanent brain damage or a persistent comatose state.

A nurse administering glucose to a patient receiving Insulin Shock Therapy in an Essex, England hospital in 1943 (left). An image of removed teeth from Henry Cotton’s The Defective Delinquent and Insane (1921) (right).
{kind=link}
{kind=link}
Because the psychiatric profession was still relatively small and the bureaucracy around mental health care was primarily concentrated in hospitals, individual doctors could often experiment to see what would work.
Henry Cotton, a doctor at New Jersey State Hospital from 1907 to 1930, for example, believed that mental illness was the product of untreated infections in the body: he removed patients’ teeth, tonsils, spleens, and ovaries to try and ameliorate their symptoms. Mortality for these procedures was 30 to 45 percent.
Perhaps the most extreme example of a physical treatment was lobotomization. Developed by Antonio Egas Moniz, doctors severed connections between the prefrontal cortex and the rest of the brain by either drilling through the skull or inserting an implement past a person’s eye. Around 40,000 lobotomies were performed in the United States. A few individuals recovered or showed improvement, but most showed cognitive and emotional declines, while others became incapable of caring for themselves or died.

{kind=link}
None of these treatments arrested the alarming growth of patient populations in state institutions. In the case of insulin therapy or Dr. Cotton’s surgeries, we can see now there was no connection between the treatment and mental illness. Such treatments simply traumatized patients or inflicted lasting physical harm.
Patients vs. Budgets
The Great Depression placed further strain on these institutions and hospitals became dangerously overcrowded. States reduced appropriations for their major state hospitals while counties began sending even more people to state institutions. Spending on patient care varied widely across the nation. In 1931, New York spent $392 per capita on hospital maintenance, Massachusetts $366, Oregon $201, and Mississippi only $172.
Under these conditions, the quality of care deteriorated. For instance, Creedmoor Hospital in New York made headlines in 1943 following an outbreak of amoebic dysentery among patients. In Salem, Oregon, a patient accidentally put rat poison in the scrambled eggs in 1942, killing 47 people and sickening hundreds—a painful example of how sloppily the hospital was run.
In 1948, the journalist Albert Deutsch released a book called The Shame of the States in which he cataloged various abuses he witnessed in state hospitals: overcrowding, beatings, and a near absence of rehabilitative therapy.
The movie The Snake Pit (1948) brought these conditions to life, showing the different levels of a hospital, including the “snake pit,” where patients deemed beyond recovery were abandoned in a padded cell.

Journalist Albert Deutsch published a catalogue of abuses in state hospitals in 1948 (left). One of the images in Deutsch’s The Shame of the States of an overcrowded day-room in a Manhattan asylum (center). The 1948 film The Snake Pit depicted a semi-autobiographical story of a woman in an insane asylum who could not remember how she got there (right).
{kind=link}
Such attention, along with World War II, mobilized public support for reforms to mental health care. The sheer number of potential soldiers rejected for service on psychiatric grounds—1.75 million—shocked the public. Then, the large number of psychological casualties among men, many of whom suffered from what we now would call Post-Traumatic Stress Disorder, also suggested that environmental stress could contribute to psychological problems.
Deinstitutionalization: Medicines to the Rescue?
The continual (and, many feared, financially unsupportable) growth of patient populations, the shameful conditions of the hospitals, and the postwar interest in psychiatry created a groundswell for reform.
The signing of the National Mental Health Act in 1946 and the subsequent creation of the National Institute of Mental Health (NIMH) signaled that the federal government would play a larger role in overseeing mental health and soliciting the input of psychiatrists. By the mid-1950s, NIMH studies were calling for community care rather than hospitalization.

A poster presentation at the Minneapolis Health Fair in 1944.
The postwar period also saw the arrival of psychotropic medications and treatments. Thorazine became the first antipsychotic, making its way to the United States in 1954, and soon proving effective at alleviating certain symptoms. Effective medications raised the possibility of moving people out of the hospitals permanently.
Generally, deinstitutionalization began around 1955 as the number of people in hospitals began to decline afterward. New York became one of the first states to reform its mental health care system, beginning with its Community Mental Health Act in 1954. This act provided funding to outpatient clinics for patients to visit for therapy or medications. Other states followed suit.

1955 and 1956 advertisements for the antipsychotic drug Thorazine in Mental Hospitals magazine.
State governments proved unwilling to pay for extensive networks of clinics, however, and counties resisted the financial responsibility. California’s mental health act asked families of those in treatment to pay, thus minimizing the tax burden. Complaints about state hospital systems frequently circled back to its cost to the states, especially as patient rosters grew longer.
At the same time, other reformers were optimistic about new, in-hospital treatments such as milieu therapy. At its core, milieu therapy tried to divide patients into small “communities” that would make decisions about collective behavior and daily life in the hospital wards. It aimed to create collaborative patient-staff relationships and teach people how to live independently.
An Expanded Role for the Federal Government
The Kennedy Administration and the Great Society helped to break the financial logjam at the state level and give politicians the monetary support to shutter their hospitals. In 1963, the president called for a new approach that would allow mentally ill individuals to live successfully in their communities.

The Kennedy Family at Hyannis Port, MA in 1931 with Rosemary Kennedy on the far right (left). President John F. Kennedy signing the Mental Retardation Facilities and Community Mental Health Center Construction Act in late October 1963 (right).
{kind=link}
{kind=link}
Kennedy proposed a program to “assist in the inauguration of a wholly new emphasis and approach to care for the mentally ill,” he said in a speech. “This approach relies primarily upon the new knowledge and new drugs acquired and developed in recent years which make it possible for most of the mentally ill to be successfully and quickly treated in their own communities and returned to a useful place in society.”
Kennedy’s sister Rosemary had been born with a mild intellectual disability and in her teenage years reportedly became difficult to manage. Fearing that Rosemary’s behavior might embarrass the family, Joseph Kennedy, Sr. had her lobotomized, hoping to improve her symptoms. Instead, it left her an invalid hidden away in an institution. Her father reportedly never visited her again.

Kennedy’s bill offered $150 million in grants for states to construct community mental health centers (CMHCs), with the federal government sharing between one- and two-thirds of the total cost. The centers would be required to offer inpatient services, outpatient services, partial hospitalization, 24-hour emergency services, and educational work. The bill called for 2,000 CMHCs to be built by 1980, with the goal of rendering most state hospitals obsolete. Signing the Community Mental Health Act was one of Kennedy’s last acts; he was assassinated a few days later.
The Community Mental Health Act was the brainchild of just a few psychiatrists: Robert Felix, Stanley Yolles, and Bertram Brown. They categorically opposed any significant role for state hospitals in the future, and largely bypassed the directors of state mental health programs. Felix hoped that his CMHCs would have a preventive effect on mental illness. Certainly, Kennedy seemed optimistic about the prospects of medications, which he said could successfully and quickly treat people to return them to a “useful place in society.”
Felix’s belief that the CMHCs would prevent mental illness was unfounded; there is little evidence that they had any positive effect. Underfunded from the beginning, by 1980, only 754 of the promised centers were in operation. But the CMHC program did have the effect of undermining the role of hospitals in mental health care.
The states, in turn, had an ambivalent relationship with the CMHCs, in part because the funding structure demanded that states pay increasingly more for the centers. Because of that, many CMHCs sent patients requiring significant care back to the hospitals. Absent a suitable number of centers, states fell back on developing aftercare and clinics, which were spotty at best.

Originally known as the Great Asylum for the Insane, Agnews State Hospital in Santa Clara, CA opened in 1885 and closed in 1998 (left). Built after World War II, the Demented Men’s Building at Agnews State Hospital (right) was an attempt to move toward preparing patients to leave the hospital.
{kind=link}
Other federal programs had the effect of further emptying the state institutions. Medicare provided funds for the elderly to be treated in nursing homes rather than hospitals. In 1972, Social Security was modified so that payments could be made to individuals not living in a hospital, to encourage people to live independently. Medicaid also was designed to encourage states to move people out of hospitals and into smaller facilities. States could only be reimbursed for expenses if individuals were living in a facility with 16 or fewer beds.
States Get Out of the Business of Mental Health, or Try To
Under the new federal strictures, states had incentives to close their asylums. California, under Governor Ronald Reagan, became a leader in deinstitutionalization and set an example for other states.
Yet California’s deinstitutionalization also reveals the dual impulses that drove politicians. Nick Petris, a state legislator, worked to limit the number of involuntary commitments by passing laws that restricted how people could be sent to a hospital. Once those hospitals were closed, Petris hoped the funds would follow the patients. Instead, in the landmark Lanterman-Petris-Short Act that Petris authored, Governor Reagan diverted the funds that were supposed to pay for patient care at the county level into the state’s general fund.

A graph depicting inpatient psychiatric beds by type from 1970 to 2002.
Even states that had historically been sympathetic to funding mental health care followed the pattern. New York counties resisted opening centers because of the funding formula the state had instituted. In Massachusetts in the mid-1970s, under Michael Dukakis, hospital closures accelerated partly out of the need to slash budget expenditures. Once budgets were slashed, many hospitals saw their quality of care decline further, leading to more demands that they be emptied and closed.
Decisions in both the state and federal courts also changed how commitment worked, further shrinking state hospitals. The culminating Supreme Court decision, O’Connor v. Donaldson (1975), held that people not deemed to be a threat to themselves could not be hospitalized against their will.

After the 1975 decision, hospitals became (as they remain today) forensic institutions for the most part, housing criminal offenders or individuals awaiting trial. As a result, from 1970 to 2016, the number of inpatient psychiatric beds in the United States declined from 413,000 to 37,679.
Deinstitutionalization: What Happened to the People?
Many individuals’ quality of life improved after leaving the hospitals—a process that accelerated from the 1950s. Medications significantly enhanced their ability to manage their symptoms.
Once people exited hospitals, their destinations varied. Reformers hoped that they would go home to families, but in many cases, people had no family connections. Without family to support them, and often having never lived independently, people with mental illness often turned to the federal government for support.
The number of halfway homes exploded. Often these group homes were opened by ex-hospital staff. They tended to cluster in low-rent areas of major cities, partly because that was where the operators could afford to run them, and because neighborhood associations were generally unwilling to accept group homes in safer, more affluent neighborhoods.
The quality of these homes could vary dramatically: most states paid the operators of such homes by the head, which gave them incentives to maximize profits. Horror stories became distressingly common from the 1970s onward. A house fire in Worcester, MA, killed seven people in a group home, while nine people in Mississippi were found living in a 10- by 10-foot shed with no running water and only two mattresses. The worst of these houses came to resemble the hospital wards people had left, with drab environments and limited contact outside the house.

The promise of medications to “cure” mental illness has also faltered. Medications have proven variable in their efficacy from person to person. They might be useful in controlling one set of symptoms while failing to address another.
They also frequently involve a number of side effects, the most widely known of which is the “Thorazine Shuffle” (a combination of the tranquilizing effect of drugs with restless legs, making consumers walk with a shuffling gait) but others include severe weight gain, facial tics, and muscle spasms.

{kind=link}
Medications must be taken consistently to remain effective. This helped to reinforce the so-called “revolving door” of mental health in which a person discontinues a medication, decompensates psychiatrically, is arrested or hospitalized, recovers, and repeats.
Policy makers never considered these complications of drug-based solutions. Doctors were often circumspect about the effectiveness of medications, but professional medical input into federal government programs was limited.
The era of deinstitutionalization reached its denouement with Reagan’s 1981 Omnibus Budget Reconciliation Act. It repealed federal funding for CMHCs, transformed other federal aid to the states into block grants, cut the dollar outlays by as much as 30 percent, and left the states with broad discretion over how to spend the money. By the mid-1990s, hospitals had mostly shrunk to their present size.
Mental Health Today
It would be a mistake to paint deinstitutionalization as a through-and-through failure.
The hospitals that existed in the 1940s were often abusive, and many people today can live their lives in a way they might only have dreamt of a century ago. Hospitalization was not the best option for people with mild symptoms that could be managed through medications.
Yet many people were left behind as well, either on the street or in jails and prisons.
What is striking about the legacy of deinstitutionalization is how much of it was motivated by financial opportunism on the part of the states. Over the course of the 20th century, states’ elderly patients could have their treatment funded by Medicaid, hospitals could be shrunk and staff ratios could be improved without having to actually spend more money, clinics would be cheaper to run than hospitals, and medications would maybe even obviate the need for any treatment at all.
This focus on reducing funding outlays helps to explain the limitations of this brand of reform: it was supposed to be cost-effective. Those individuals who required more support once they left the hospitals found themselves abandoned.

The creation of a large, indigent class of people with mental illnesses was not inevitable from a policy perspective. Studies from the United States, Germany, and Switzerland, among other countries, have confirmed that even people who have been institutionalized most of their lives and who have experienced severe mental illness for years on end can live independently if they have certain supports available: housing, aftercare, support networks, and jobs.
However, in the United States, those supports frequently have not existed, or in certain cases, have been eroded or ended once people returned to the community. Psychiatrists such as Robert Felix underestimated the extent to which they would be necessary, and politicians at the state and federal level were unwilling to spend the money.
As the mental health system again reemerges in public and policy discussions in the wake of another mass shooting, the question remains: Is there a link between closing the hospitals and mass shootings? In all likelihood, no. Americans do not suffer from higher rates of mental illness than other people in the world.
While not all agree, the general consensus among psychiatrists is that there is no meaningful link between mental illness and the number of mass shootings. Representing this majority scientific view, epidemiologist Matthew Miller argues that the number of mass shootings in the United States has far more to do with the availability of guns. In contrast, some psychiatrists such as E. Fuller Torrey maintain that there are certain links between untreated mental illness and violence (although Torrey’s conclusions are controversial and are challenged by other experts).

President Trump has recently suggested that the United States needs more hospitals and asylums to prevent future shootings. Whether this proposal is serious is up for debate. Current commitment laws would make it difficult to hold people against their will en masse.
To respond in this manner would simply reframe mental illness as a problem of violence, not of mistreatment and maltreatment of Americans with mental illness. Such a program would be unlikely to fix a broken system.
As for the state of Florida, legislators are trying to pass additional appropriations for mental health care. The long history of American approaches to mental illness should leave us doubtful that the funding would remain for long.